People have been "grinding my gears" by conflating carbohydrates with sugars. All sugars are carbohydrates, but not all carbohydrates are sugars. See Carbs Carbs Carbs. to find out about the five basic different types of carbohydrates.
Krauss et al has been "at it" again. In Separate effects of reduced carbohydrate intake and weight loss on atherogenic dyslipidemia, at the bottom of Table 1 is "carbohydrate, 50% simple and 50% complex". The carbohydrates consisted of half simple (probably fructose, as that has the worst effect on particle size) and half starches (probably maltodextrin, as it rapidly hydrolyses into glucose).
The effect of such a sugary diet is as follows:-
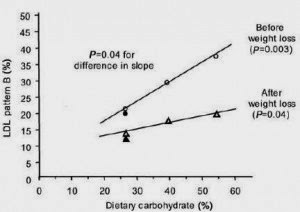
The percentage of pattern B (small, dense) LDL particles increases significantly in proportion to the percentage of Dietary "carbohydrate". The implication of this study (also A very-low-fat diet is not associated with improved lipoprotein profiles in men with a predominance of large, low-density lipoproteins ) is that high-carb, low-fat diets are atherogenic.
I call "Shenanigans".
A high sugar diet is atherogenic, but carbohydrates from potatoes, rice, sweet potatoes/yams & beans (if not overcooked), actual whole grains (i.e not flour) & whole fruits aren't.
15 comments:
Nigel, you sound like Dr. Robert Lustig and Dr. Richard Johnson. We do need proper experiments looking at food quality.
I sound like Dr. Robert Lustig? Nooooooooooooooooooooooooooooo!
See http://www.alanaragonblog.com/2010/01/29/the-bitter-truth-about-fructose-alarmism/ and http://www.alanaragonblog.com/2010/02/19/a-retrospective-of-the-fructose-alarmism-debate/
Please read all (well, most anyway) of the comments. I left comments broadly supportive of Dr. Lustig, but was unable to back up my case with quality evidence.
I am now of the opinion that fructose is a problem in certain doses and in certain contexts. A diet of mostly crap-in-a-bag/box/bottle meets those criteria.
P.S. You are white-listed, so any future comments will appear immediately.
Nigel, I was referring to the sugar (in general) hidden within experiments, not the fructose-phobia stuff. A true honor to be white-listed.
Ah! Anyway, the above links are still interesting. I white-list most commenters as it saves me from having to moderate comments using my phone, as I'm out most evenings doing music-y stuff.
Nige, nice blog. I agree that all carbs are not created equal, however, have to disagree with your statement that potatoes, rice, beans and whole fruits aren't atherogenic, because that is NOT what I see clinically. Patient's bring in their food diaries to me and I evaluate their sdLDL particles every three months. ANY potatoes, ANY rice, and MOST fruit will raise the sdLDL particle number and their CIMT studies show progression of atherosclerosis. The reason is that EVERY one of these will raise the triglyceride level. I've been seeing this clinically for the last 5 years.
Hi,
I actually wrote (emphasis, mine) "...carbs from new potatoes (especially if eaten cold), Basmati rice
(especially if eaten cold), sweet potatoes, beans & whole fruits
aren't"
Were your patients eating potatoes as per my above statement? Cooked potatoes can have a high GI unless correctly prepared (cooked al dente, so as to not raise the GI too much). Subsequent refrigeration forms RS3 (retrograde starch), which drastically lowers the GI. Ditto for rice. Basmati rice has the lowest GI of all the rice varieties.
What sort of beans were your patients eating? If beans are overcooked, their GI approaches 100 (on the glucose=100 scale). Baked beans are overcooked in a sugary sauce.
What sort of fruits were your patients eating? Some fruits are sugarier than other.
My statement was aimed at the general population, rather than people with severe insulin resistance (IR) or other metabolic derangements. People sick with IR etc (i.e. your patients) need to restrict carbohydrates more than healthy people. Have you managed to reverse IR in your patients? Have you read http://nigeepoo.blogspot.co.uk/2011/02/insulin-resistance-solutions-to.html ?
Anyway, thanks for your kind words. You are now white-listed, so any future comments from you will appear immediately.
Whether new potatoes, rice or fruit, cold or hot, Glycemic index means absolutely nothing (because our bodies do not respond like bomb calorimeters) when it comes to the formation of cholesterol and triglycerides (hence, one's atherogenic effect). A carbohydrate is a carbohydrate and will stimulate an insulin response, no matter whether it occurs in the first 30 minutes or 2 hours later. What matters is whether, and how fast, ones gut breaks down the bonds between glucose molecules. That's why physicians who understand lipogensis and lypolysis don't even look twice at glycemic index any more. Fructose still stimulates triglyceride production even though it is metabolized through the liver and then has a secondary stimulus to insulin. A blanket statement that "carbs from new potatoes (especially if eaten cold), Basmati rice (especially if eaten cold), sweet potatoes, beans & whole fruits aren't" atherogenic is absolutely false.
If that's the case, then how come populations that eat sweet potatoes/yams as their staple diet (providing ~80% energy from carbs) are slim and don't have high fasting insulin? Because they're not insulin resistant, that's why. Ditto for other "Blue Zone" populations.
The reason so many Americans are insulin resistant is partly due to all of the junk that they eat (thanks to aggressive marketing) and partly due to their modern lifestyles full of labour-saving gadgets including cars.
Carbohydrates are only a "problem" for insulin resistant people. I used to be severely insulin resistant. My OGTT result after 2 hours was 8.7mmol/L in 2003. Having discovered & rectified the main cause (Vitamin D deficiency), my OGTT result after 2 hours was 3.9mmol/L in 2006. I no longer have to drastically cut my carb intake to achieve weight loss & normal TG's. This is the way forward. I still prefer to eat only unrefined carb sources.
Anyway, I'm getting frustrated with discussing complicated concepts 140 characters at a time on Twitter. Would you like to continue the discussion here?
So, where were we?
Hi Nigel, if math says Dir-LDL, LDL-P, s-LDL-P equally predict risk, why does offspring cohort data show that LDL-P better predicts risk? I understand the math in a closed system.
Populations that live off of 80% of energy from carbs are slim because they're not taking in large amounts of fat. How do you know they done't have high fasting insulin? Many of the vegetarians I see in my office have high insulin loads and are metabolically sick. Again, blanket statements don't work.
The maths doesn't say that. The maths says that LDL level, LDL particle size & LDL-P are related to each other. That doesn't make them equivalent.
Your patients are Americans, yes? As such, they have a completely different lifestyle to islanders that have to walk everywhere and probably don't even have a TV. I've read a study on PubMed about them, but I can't recall the title off the top of my head.
Right, they are different. My thought is that there are factors beyond the math that make them different. Nigel, you are clever.
Nigel, We are all nerds and lovin' every moment!
The LDL-P test created by NMR Liposcience has become a most popular test both clinically and in research. They invented particle counting, emphasize it and we all find it rather ingenious. Less emphasis on particle size however.
I miss the days when I did VAP and Berkeley advanced lipid testing in our office. These labs place emphasis on cholesterol quality, particle size and sub classes (Berkeley does seven sub-classes of LDL-C). Both these labs also measured direct LDL-C and or direct ApoB, how simple.
We need experiments looking at cholesterol quality and outcomes as there may indeed be a link.
Post a Comment